
1. Introduction
2. AIDS and HIV: the missing link
3. The nonexistent virus
4. AIDS is not contagious
5. Africa: fact vs. fantasy
6. Poisoning the patients
7. Challenging the establishment
8. Risk factors and survival
9. Sources
‘There is no question HIV is the cause of AIDS. Anyone who gets up publicly and says the opposite is encouraging people to risk their lives.’ – David Baltimore, Nobel laureate
‘Years from now, people looking back at us will find our acceptance of the HIV theory of AIDS as silly as we find the leaders who excommunicated Galileo.’ – Kary Mullis, Nobel laureate
Contrary to popular belief, Acquired Immune Deficiency Syndrome (AIDS) is not a global pandemic caused by the human immunodeficiency virus (HIV); rather, it is one of the biggest and deadliest medical scandals of modern times. There is no convincing evidence that ‘HIV’ plays any role in impairing the immune system, is transmitted sexually, and is the sole cause of AIDS. In fact, there is no compelling scientific evidence that ‘HIV’ even exists: pure HIV particles have never been isolated from supposedly infected individuals using standard scientific procedures.
HIV/AIDS is above all a multibillion dollar industry, in which so many scientists and organizations have acquired a stake that the views of researchers who challenge the orthodox position are vigorously suppressed. According to the mainstream media, high-profile science journals and AIDS propagandists, there is ‘overwhelming evidence’ that HIV causes AIDS, and those who deny this are a public health menace and deserve to be silenced. But it is a telling fact that all the catastrophic predictions made since the early 1980s on the basis of the HIV=AIDS=Death dogma have failed to materialize.
In the early days of rampant hysteria, it was predicted that AIDS in the West would spread from bisexual men to female prostitutes and then into the general population, and that 1 in 5 heterosexuals could be dead within three years. In 1987 the US President’s AIDS Commission stated that by 2001 there could be 10 billion people infected – a number far greater than the world population, meaning that the human race could become extinct. Needless to say, nothing remotely like this has happened. In the West, AIDS is still found mainly in the original high-risk groups: gay men and drug addicts.
According to UNAIDS, 630,000 people died of AIDS in 2023, 1.3 million people became ‘newly infected with HIV’, and 39.9 million were ‘living with HIV’, of whom 5.4 million were unaware that they were ‘infected’. A total of 42.3 million people have allegedly died of AIDS since the early 1980s. It should be borne in mind that such statistics are inflated estimates based on computer models: the higher the numbers, the higher the funding. In 2007, UNAIDS reduced its estimate of new ‘HIV’ infections by 40%, and reduced the total number of infected people from 40 million to 33 million, while other experts put it at 25 million (Timberg, 2007).
In the name of fighting HIV/AIDS, hundreds of thousands of lives have been destroyed. People who test positive on the highly dubious ‘HIV tests’ – including those who are otherwise perfectly healthy, among them babies and young children – are treated with extremely toxic drugs, which can cause several AIDS-defining conditions, while giant pharmaceutical companies rake in the profits.
‘HIV’ is generally believed to be 100% lethal if left untreated. In the early 1980s, it was claimed that death followed only months after infection, but this ‘latency period’ was later increased to 10, 20 or even 30 years. The view nowadays is that many HIV-positive people can survive indefinitely as long as they keep taking antiretroviral drugs to manage chronic infections. People are also encouraged to take preexposure prophylaxis (PrEP) pills, which supposedly prevent infection with HIV. However, many HIV-positive people have survived for decades after refusing to take the official drug treatments. A major reason why AIDS deaths have fallen by over half since the mid-2000s is that patients are now given less toxic drug cocktails and dosages. Another reason is that the definition of AIDS has been expanded and people can be classed as HIV-positive even if they are completely healthy.
‘HIV’ is said to be a retrovirus, but no other retrovirus is believed to kill cells. Since it is difficult to detect any significant signs of HIV in the bodies of AIDS patients, people are tested for the presence of antibodies to HIV, but there is no evidence that there are any antibodies specific to HIV. Moreover, in the case of many other supposed viruses, the presence of antibodies is regarded as a sign that the virus in question has been defeated and the person concerned is immune.
The mainstream position is that HIV is a new kind of invasive retrovirus with unique properties, and behaves in ways that no one can explain, despite over 570 billion dollars being spent on AIDS research in the United States alone. But, as we will see, there is no need to invoke ‘HIV’ to explain immune deficiency. In the developed countries, drugs and certain sexual practices are among the main factors causing ‘AIDS’, while in the developing countries the key factors are malnutrition, poverty and poor sanitation.
In 1981 two rare diseases – PCP (a fungal-related pneumonia) and Kaposi’s sarcoma (a skin cancer) – began to increase rapidly among young, sexually promiscuous, drug-using homosexual men in several American cities. The name Gay-Related Immune Deficiency (GRID) was coined, but when gay leaders objected, it was changed to Auto-Immune Deficiency Syndrome (AIDS). The idea that the body was destroying its own immune system was soon dropped, but since the acronym (AIDS) had already caught on, it was retained, with the name being changed to Acquired Immune Deficiency Syndrome.
Since then, many more ‘AIDS indicator diseases’ have been added. The US Centers for Disease Control (CDC) currently lists 27 familiar illnesses and conditions as AIDS, but only if they occur in people who test ‘HIV-positive’. They include yeast infection, herpes, diarrhoea, some pneumonias, certain cancers, salmonella and tuberculosis. This means, for example, that people who die of tuberculosis are said to have died of AIDS if they are HIV-positive, but to have died of tuberculosis if they are not. Heroin addicts get pneumonia, which is not surprising since the drug damages the lungs. But if a heroin addict tests HIV-positive, the cause of their lung disease is attributed to ‘HIV’ and they become an AIDS case. ‘AIDS’ is clearly an artificial construct.
‘HIV’ is the only virus which is said to cause a group of diseases that are believed to be caused by other viruses and bacteria, rather than causing its own disease (in reality, bacteria and so-called viruses are never the root cause of disease; see Reclaiming our health). Moreover, AIDS patients do not have any one of the 27 AIDS-defining conditions in common. And some AIDS diseases, including dementia, wasting syndrome and cancers, are neither caused by nor necessarily associated with immune deficiency.
If HIV causes AIDS, the prevalence of HIV and AIDS should be closely correlated – but they are not. In the United States, HIV infections remained more or less constant at about 1 million after widespread testing began in 1985, whereas AIDS cases increased from 1981 to 1992 and then declined. HIV testing by the US military consistently reported near equal numbers of HIV-positive results among male and female new recruits, yet 80% of AIDS patients in the US and Europe are males. Between 1981 and 2000, the ratio of black Americans to white Americans reported with AIDS trebled, while the ratio of positive HIV-tests in the two groups remained the same (Bauer, 2006c).
The CDC has expanded its definition of AIDS several times since 1981, with each change boosting the number of AIDS cases. The number of AIDS-defining conditions was increased to six in 1985, 23 in 1987, and 26 in 1993. In 1993 the definition was also expanded to include people who have no illness but have a CD4+ T-cell count of less than 200 cells per millilitre of blood (T-cells are a type of white blood cell forming part of the immune system). This caused the number of HIV cases in the United States to double overnight.
Thereafter, over half of all new HIV cases each year were among people who were not ill, resulting in a lower death rate. However, Canada, like most of Europe, did not recognize the American T-cell count criterion for AIDS. This meant that more than 25% of all the people in the United States ever diagnosed with HIV could be cured instantly simply by crossing into Canada. A further condition for an AIDS diagnosis was that there should be no other known cause of the ‘immune deficiency’, but US health authorities dismissed drug abuse as a possible cause.
In most of Africa, World Health Organization (WHO) guidelines allow patients to be diagnosed with AIDS if they have a combination of three or four symptoms such as chronic diarrhoea, prolonged fever, persistent cough, weight loss of 10% or more, and generalized itching. In most African countries no HIV test is required.
The proclaimed link between HIV and AIDS dates from 1984. In April of that year, Robert Gallo, a researcher at the National Institutes of Health (NIH), called an international press conference together with the US Department of Health and Human Services, at which he announced his discovery of a new retrovirus described as ‘the probable cause of AIDS’. This announcement was made before publication of any scientific evidence supporting the virus theory. Later the same day he filed a patent for the ‘AIDS test’.
By the following day the media were calling HIV (then known as HTLV-III) ‘the virus that causes AIDS’, and the presence of HIV (or rather alleged antibodies to it) quickly became part of the definition of AIDS. Many researchers who had previously favoured the hypothesis that recreational drug use was a major cause of AIDS dropped the hypothesis to work on the new ‘AIDS virus’, because that’s where the money was.
The first publication from Gallo’s group in support of the theory that HIV causes AIDS reported finding that 18 out of 21 ‘pre-AIDS’ patients (86%) tested HIV-positive, but only 26 of 72 people (36%) who had full-blown AIDS. This makes no sense if HIV is the cause of AIDS. Nor was any proof offered that HIV differed from other retroviruses, which are considered to be harmless and unable to kill cells. The HIV=AIDS hypothesis received no widespread critical scrutiny because it fitted in with the prevailing microbe-hunting mentality. All funding for research into other potential causes came to an abrupt halt, and only discussions on how HIV causes AIDS were tolerated, but not on whether HIV causes AIDS or even exists.
A Congressional investigation later found that Gallo had presented fraudulent data in his 1984 HIV papers, and that the virus he claimed to have discovered was the same one (known as LAV) that he had been sent by Luc Montagnier of the Pasteur Institute in France, whose team had discovered it in 1983. The French and American governments finally negotiated a compromise, with Montagnier and Gallo sharing credit as co-discoverers of HIV and ownership rights to the ‘HIV test’. Gallo and his collaborators received $100,000 annually in royalties. In 2008 Montagnier and his colleague Françoise Barré-Sinoussi were awarded a Nobel Prize for the discovery of HIV. However, both Montagnier and Gallo acknowledged that their laboratories never isolated pure HIV particles, and both came to doubt whether HIV was the sole cause of AIDS.
Kary Mullis, who won the Nobel Prize for Chemistry in 1993 for inventing the polymerase chain reaction (PCR) technique, tried to find out why scientists had become so convinced that HIV caused AIDS. He argued that the detection of alleged antibodies to HIV in a person suffering from AIDS does not prove that HIV causes AIDS.
Antibodies to viruses had always been considered evidence of past disease, not present disease. Antibodies signalled that the virus had been defeated. ... There was no indication in these papers [by Montagnier and Gallo] that this virus caused a disease. They didn’t show that everybody with the antibodies had the disease. In fact, they found some healthy people with antibodies. (Mullis, 2000, p. 173)
Mullis proceeded to ask AIDS experts he met at conferences to tell him in what article he could find the proof that HIV causes AIDS.
Everyone said something. Everyone had the answer at home in the office in some drawer. They all knew and they would send me the papers as soon as they got back. But I never got any papers. Nobody ever sent me the news about how AIDS was caused by HIV. (p. 174)
Finally, he had the opportunity to ask Montagnier himself:
With a look of condescending puzzlement, Montagnier said, ‘Why don’t you quote the report from the Centers for Disease Control?’
I replied, ‘It doesn’t really address the issue of whether or not HIV is the probable cause of AIDS, does it?’
‘No,’ he admitted, no doubt wondering when I would just go away. ...
‘Why don’t you quote the work on SIV [simian immunodeficiency virus]?’ the good doctor offered.
‘I read that too, Dr. Montagnier,’ I responded. ‘What happened to those monkeys didn’t remind me of AIDS. Besides, that paper was just published only a couple of months ago. I’m looking for the original paper where somebody showed that HIV caused AIDS.’
This time, Dr. Montagnier’s response was to walk quickly away to greet an acquaintance across the room. (Duesberg, 1996, pp. xii-xiii)
Mullis became a member of the Group for the Scientific Reappraisal of the HIV/AIDS Hypothesis, which received the support of 2897 professionals. He argued that retroviruses are everywhere, and are passed from mother to child, but they’ve never been shown to have killed anyone (the word retrovirus is therefore misleading). He comments wryly: ‘HIV didn’t suddenly pop out of the rain forest or Haiti. It just popped into Bob Gallo’s hands at a time when he needed a new career’ (Mullis, 2000, p. 178). Gallo had previously been involved in the search for genes that cause cancer (oncogenes), and, like numerous others researchers (including Montagnier), had become frustrated by the lack of success.
All the old virus hunters from the National Cancer Institute put new signs on their doors and became AIDS researchers. Reagan sent up about a billion dollars just for starters, and suddenly everybody who could claim to be any kind of medical scientist and who hadn’t had anything much to do lately was fully employed. They still are. (p. 177)
As HIV came to be automatically equated with AIDS, anyone testing HIV-positive qualified as a disaster victim eligible for treatment at public expense, which meant lucrative consultation and testing fees, and treatment with drugs that have proved highly profitable for the pharmaceutical industry. County health authorities received $2500 per year for every reported AIDS case.
The ‘evidence’ that HIV causes AIDS is purely epidemiological: persons who test HIV-positive often develop AIDS and those who test negative usually do not. But since AIDS is now defined as requiring a positive HIV test, it’s hardly surprising that everyone with AIDS is HIV-positive. Only about 50% of HIV-positive people ever become ill (those who don’t are labelled ‘asymptomatic carriers’), and by no means all patients with AIDS symptoms test HIV-positive. The scientific literature documents 4621 confirmed cases (to 1992) of HIV-free people dying of AIDS symptoms. To preserve the dogma that HIV causes AIDS, a new condition was invented to cover these cases – ‘idiopathic CD4-lymphocytopenia’. Idiopathic means ‘no known cause’, so this is just a scientific-sounding way of saying ‘we haven’t got a clue’, but it has the advantage of allowing these paradigm-busting cases to be excluded from official AIDS statistics.
Strictly speaking, there is no such thing as a test for HIV/AIDS. All the test kits are accompanied by disclaimers in which the manufacturers warn that the tests should not be used to diagnose HIV infection or AIDS. The ELISA test looks for antibodies that are assumed to be specific to ‘HIV proteins’ (antigens) in a person’s blood, oral fluid or urine. If the result is positive it may be confirmed with the Western blot test, which tests blood for antibodies to various individual proteins. Such proteins include p24 and p41, but these are also found in blood platelets of healthy individuals (Goodson, 2014).
It is not uncommon for successive HIV tests of the same individual to switch back and forth between positive and negative results. ‘False-positive’ HIV tests can result from almost 70 medical conditions, e.g. a variety of ‘infections’ (including flu), flu/tetanus/hepatitus B vaccination, interferon therapy, many antibodies, blood transfusions, autoimmune diseases, haemophilia, hepatitis, herpes simplex, leprosy, malaria, certain cancers, rheumatoid arthritis, tuberculosis, and multiple pregnancies (Johnson, 1996). Anyone who produces high levels of antibodies in response to exposure to some toxin or other health challenge is at risk of testing positive. If HIV is not a real virus, all HIV-positives are false positives, though a positive antibody test may still correlate with a heightened risk of disease.
HIV tests are officially said to be 99.9% accurate, but this figure is based on circular logic: an ELISA test is considered accurate if a person who tests positive also tests positive on the Western blot; and a Western blot test is considered accurate if a person who tests positive also tests positive when retested. No HIV test has ever been scientifically validated by isolating HIV particles from the fresh (uncultured) blood plasma of people who test positive.
In some instances, the accuracy of antibody tests has been assessed by putting a tested person’s blood into a chemically stimulated cell culture, and looking for indirect evidence of ‘HIV’. The tests were then found to be between 41% and 76% accurate for people with AIDS conditions, and between 0% and 16% accurate for those with no symptoms (Philpott, 1997). In another study, 50% of blood samples from healthy dogs reacted positively on HIV antibody tests (Maggiore, 2000, p. 8).
Out of 30 or so possible retroviral proteins, about 10 were selected as being specifically from HIV and nothing else. However, this was not done by isolating HIV and showing that it contained these proteins. Instead researchers simply selected the proteins that most commonly reacted in blood samples of AIDS and pre-AIDS patients. The circular reasoning behind HIV tests can be summed up as follows:
• Take a mixture of yet to be identified proteins (in a cell culture) derived from AIDS patients.
• Add another mixture of yet to be identified antibodies (in serum) from AIDS patients.
• Designate the proteins that react as ‘HIV’ proteins.
• Designate the antibodies that react as ‘HIV’ antibodies.
Biophysicist Eleni Papadopulos comments: ‘Hence, starting with two unknowns, each unknown identifies the other. That is, antibodies identify the proteins that identify the antibodies’ (Hodgkinson, 2017).
HIV test kits are calibrated to ensure that most healthy people test negative, but there are no international standards for deciding what constitutes a positive result, and someone could switch from positive to negative simply by changing countries. For instance, someone whose test reacts to proteins p160 and p120 would be considered HIV-positive in Africa, but not in Britain. A test reaction to p41, p32 and p24 would be considered positive in Britain, but negative in Africa (Goodson, 2014).
In the ELISA test, the serum reacts with a mixture of the selected proteins to cause a colour change. But there are varying degrees of colour change, and the cutoff value between ‘positive’ and ‘negative’ is not universal but is determined by the testing venue and depends on what the test is intended for. Moreover, the serum is first diluted 400-fold, otherwise everybody would test positive.
The result of the Western blot takes the form of a series of reactive protein bands, and depending on the lab or the country in which it is located, different combinations of two, three or four bands are sufficient to diagnose HIV infection. Until 1987, a positive p24 band on the Western blot was sufficient to label someone as infected with HIV. In the United States and many other countries, a positive HIV diagnosis based on the ELISA test must be confirmed by a Western blot test. In Britain, diagnosis relies on repeat tests with various types of ELISA, as the Western blot is regarded as too unreliable.
Unfortunately, according to orthodox thinking a positive result on a nonstandardized, nonspecific HIV test used to be equivalent to a death sentence, and therefore had a devastating impact on the individual concerned. Having been told that they would die a horrible death within a few years, many people chose to commit suicide. Nowadays a positive test is taken to mean that the person concerned must take antiretroviral drugs for their rest of their life in order to survive. The Office of Medical and Scientific Justice has successfully defended more than 50 ‘HIV-positive’ individuals charged with endangering others by exposing them to possible transmission of ‘HIV’, by forcing the prosecution to acknowledge that positive ‘HIV’ tests do not prove infection (Bauer, 2017).
‘Viral load’ tests were introduced in 1999, but these, too, do not measure levels of actual virus particles in the blood. A person’s ‘viral load’ is usually determined by means of the polymerase chain reaction (PCR) technique. This multiplies billions of times small genetic segments assumed to form part of ‘HIV’ so that they become detectable, and these fragments of genetic material are then assumed to correspond to counts of actual virus.
Evidence suggests that these genetic fragments might be associated with harmless ‘human endogenous retroviruses’ or HERVs (De Harven, 2010). Such retrovirus-like particles can be produced by cells that are stressed or dying, or by cells that have been hyperstimulated to grow in cell cultures. Retrovirus-like particles can be detected in individuals with non-AIDS illnesses and even no illness. Moreover, 8% of the human genome is said to consist of endogenous ‘retroviral’ sequences (Griffiths, 2001).
Low viral loads do not correlate with high T-cell counts or good health, while high viral loads do not correlate with low T-cell counts or sickness, and have also been measured in healthy people who are HIV-negative. PCR is routinely used to diagnose HIV infection in newborn children and as justification for treating infants with potent drugs such as AZT. In June 2014 the CDC replaced the Western blot with PCR (or NAT: nucleic acid test) as the ‘gold standard’ for determining the ‘true infection status’ of individuals who have indeterminate antibody tests. Kary Mullis, the inventor of PCR, said that the conclusions being drawn from PCR tests are worthless. Some critics have bluntly characterized the viral load hypothesis as ‘a viral load of crap’.
HIV is supposed to be a lethal retrovirus that may have originated among chimpanzees in Africa. It is said to be transmitted mainly via sexual intercourse and blood, and to gradually destroy the cells of the immune system, so that victims eventually die from the inability to resist a variety of well-known diseases. There are said to be two types: HIV-1, responsible for most cases worldwide; and HIV-2, largely confined to West Africa.
A retrovirus consists of a single strand of RNA (ribonucleic acid) inside a protein shell. After invading a host cell, it is said to insert a DNA copy of its genome into that cell’s DNA, thereby modifying it. The process of converting RNA into DNA is called reverse transcription, and requires an enzyme (catalyst) known as reverse transcriptase (RT). The discovery of RT in 1970 was revolutionary, because it contradicted the official dogma that it was only possible for DNA to be converted into RNA, which then makes proteins.
RT was originally detected in cancer cells, and because these cells were assumed to have been infected by a virus, this gave rise to the concept of a retrovirus. The idea that retroviruses caused cancer was soon abandoned, but any RT activity detected was still assumed to be the work of ‘retroviruses’ (Lanka, 1995). This was a serious error, because the enzyme was later found in normal mammalian cells. Ex-virologist Stefan Lanka (1998) describes reverse transcription as a repair mechanism for chromosomal DNA, and argues that it has nothing to do with an exogenous, invasive retrovirus.
The consensus used to be that retroviruses do not kill their host cells because they cannot reproduce without them. So if HIV actually existed, it would need to have highly unusual properties to cause AIDS. The orthodox view is that, on average, ‘HIV’ only infects about 1 in 1000 T-cells (Maggiore, 2000, p. 5). Rodriguez et al. (2006) argued that HIV cannot be responsible for more than 5-8% of the loss of CD4+ immune cells that is necessary to cause AIDS. As Harvey Bialy puts it, ‘the problem of massive cell killing by minuscule amounts of virus ... remains the central unanswered question about the HIV=AIDS equation’ (2004, p. 79).
It has been claimed that HIV does not kill T-cells itself, but somehow primes them to commit suicide at a later time (Culshaw, 2007, p. 73). Some researchers have claimed that HIV exploits special receptors on human T-cells that, due to a hypothetical genetic mutation, many ‘Caucasian Europeans’ lack, but most Africans have. Curiously, many gay men also seem to possess these mysterious receptors, as do intravenous drug users and blood transfusion recipients! As Celia Farber (2006) says, ‘Such unproven hypotheses about the ingenuity of HIV proliferate in the popular and scientific media like seasonal flu.’
While immune deficiency (low levels of T4 cells) is often blamed on ‘HIV’, many AIDS researchers, including Montagnier and Gallo, have recognized that even before ‘HIV antibodies’ appear in the body, people in the risk groups may show low T-cell counts due to ‘persistent hyperactivation of the immune system’, caused by factors such as drug use, microbial infections, and exposure to semen or blood. In short, HIV is neither necessary nor sufficient to explain T4 cell decrease (Papadopulos et al., 2016).
To prove that a retrovirus exists, it has to be isolated. To do this, cell culture fluid thought to contain it is added to a test tube containing a sugar solution whose density increases from top to bottom. The tube is placed in a centrifuge and spun at ultra-high speeds for many hours, so that the particles band according to their density; ‘retroviruses’ band at a density of 1.16 g/ml. Images of the relevant band are then made with an electron microscope and its constituents are biochemically analyzed. HIV has never been successfully isolated in this way.
Montagnier and Gallo and their colleagues published five papers in Science in 1983/84 claiming to have purified HIV using density-gradient centrifugation, identified the HIV particle proteins, showed that the particles are infectious and proved HIV to be the cause of AIDS. The Perth Group has shown that all these claims are bogus and the proper control experiments were not carried out (Papadopulos et al., 2017). Lack of valid control experiments plagues HIV/AIDS research to this day.
Both Montagnier and Gallo interpreted signs of reverse transcriptase activity in their cell cultures containing samples from AIDS patients as proof that retroviruses were present. Neither research team was able to find any retrovirus-like particles in the 1.16 g/ml density band, but it was still called ‘purified virus’. Gallo did find fragments of messenger RNA (mRNA) in that band, and when the RNA was reverse-transcribed into DNA fragments, they were shown to bind to RNA obtained from ‘HIV-infected’ but not ‘uninfected’ cell cultures. This led Gallo to interpret the fragments as the genome of a new retrovirus. However:
The binding between DNA and RNA in the genetic sequences he was manipulating was to be expected, since the same material (what he was calling ‘purified virus’) was used both to obtain the ‘HIV RNA’ and to infect the cell cultures. Furthermore, since RNA of the type seen is not unique to retroviruses, he had no valid grounds for assuming the presence of a new viral agent. (Hodgkinson, 2017)
In other words, the experimental result would have been exactly the same if the material was of cellular origin, rather than being from an invasive retrovirus.
‘HIV’ has never been observed under an electron microscope in the uncultured blood plasma of AIDS patients (De Harven, 2003, 2010). Particles claimed to be HIV have only been observed in cell cultures that have been stimulated with certain chemicals or irradiated. The first electron microscope images of so-called HIV particles budding out of human cells were published in 1983 by Montagnier’s team. However, the images were obtained from a cell culture containing all sorts of contaminants, and not from the purified 1.16 g/ml band, where no retrovirus-like particles could be found, only cellular debris. Gallo, too, never published any electron micrographs of purified HIV particles.
In 1997, electron micrographs of ‘purified HIV’ were published by two groups of scientists – a US team led by Julian Bess and a Franco-German team led by Pablo Gluschankof. They admitted that the purity of ‘HIV’ preparations had not previously been verified. Eleni Papadopulos, leader of the Perth Group, comments:
In other words, for fourteen years the community of HIV experts claimed to have obtained purified HIV, and then used this material to obtain proteins and RNA as if it were unique to a retrovirus HIV, and employed it time and time again for research and producing and patenting various diagnostic tests. All without a shred of proof it contained even one particle of any description let alone a retroviral-like particle. (Papadopulos, 2006, p. 110)
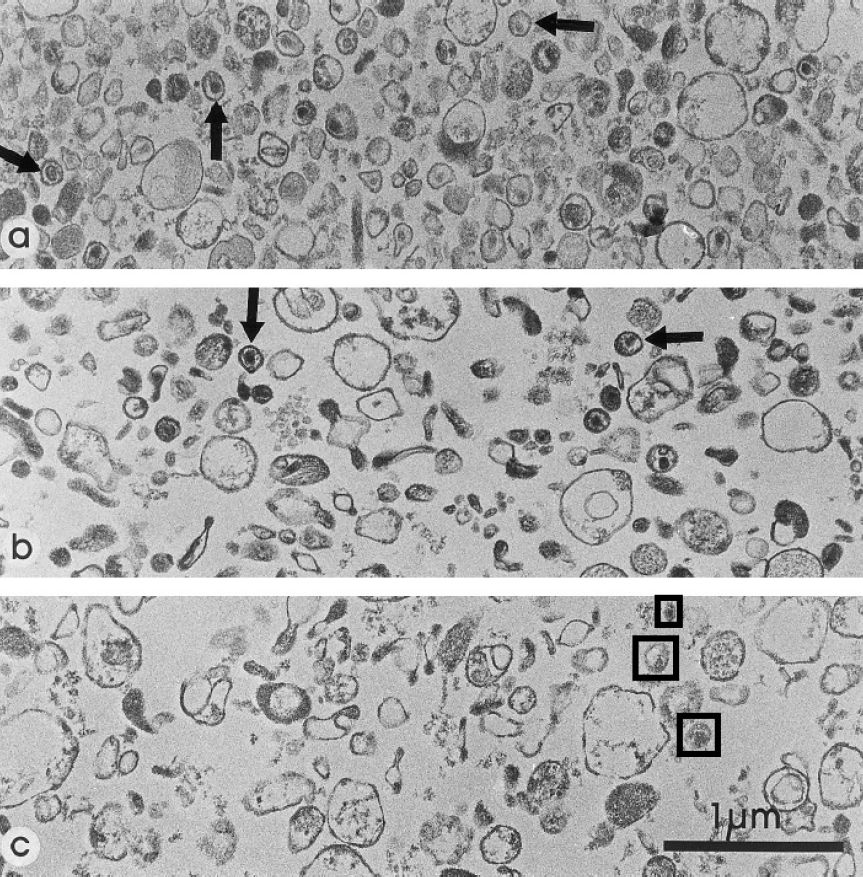
The US and Franco-German teams admitted that the vast majority of their own ‘purified’ material consisted of microvesicles (tiny fluid-filled sacs), i.e. cellular fragments, but claimed that some particles looked like retroviruses and were ‘HIV’. Yet none of these particles had all the morphological characteristics of retroviruses, or even their principal characteristics: a diameter of 100-120 nanometres (officially reduced to 80-100 nm in 2000), and surface spikes and knobs (essential for infectivity). In the Franco-German study the average ‘HIV’ diameter was 140 nm and no particles were smaller than 120 nm. In the US study the corresponding dimensions were 234 nm and 160 nm – too large to be retroviruses (Papadopulos et al., 2017).
None of the electron micrographs published by Gluschankof et al. (1997) shows purified ‘HIV’. The particles marked by arrows in the upper two images (a and b) are supposedly HIV-1; the other particles are cellular microvesicles. The third image (c) is from an ‘uninfected’ cell culture, but the particles in black boxes resemble the alleged ‘HIV’ particles.
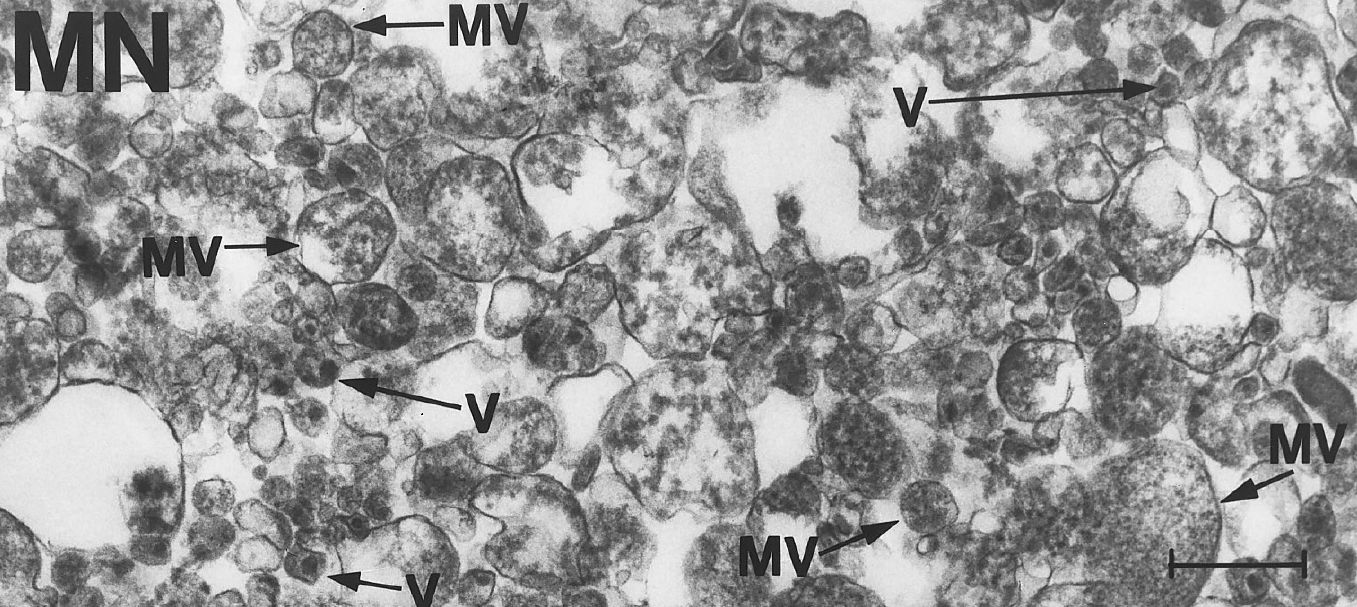
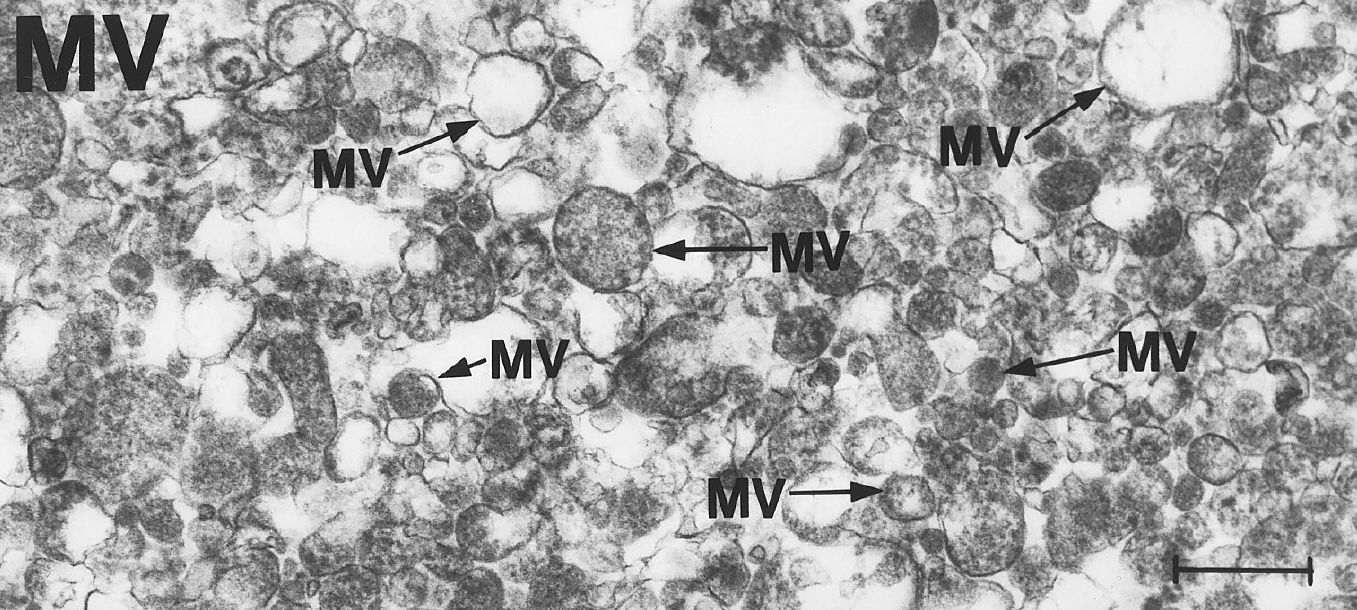
Electron micrographs published by Bess et al. (1997). Particles marked ‘MV’ are said to be normal microvesicles and those marked ‘V’ are said to be HIV. The top image is from an ‘infected’ cell culture, and the lower one is from an ‘uninfected’ cell culture. However, the latter is not a valid control experiment because, unlike other cultures, it was not irradiated, and radiation can cause the appearance of retrovirus-like particles.
There is no agreement on what genus or even subfamily of retroviruses ‘HIV’ belongs to. It has been assigned to the type-C genus (e.g. by Montagnier in 1983 and Gallo in 1984) and the type-D genus (e.g. by Montagnier in 1984), and nowadays it is generally regarded as belonging to the lentiviruses genus. Types C and D belong to a different subfamily than do lentiviruses. This is like saying that a mammal is simultaneously a human, a chimpanzee and an orangutan.
None of the supposed HIV particles in the above images show the cone-shaped core, lateral bodies and surface knobs characteristic of lentiviruses. The knob/spike count of ‘HIV’ has been claimed to be 80, 72, approximately 14, an average of 0.5, possibly zero, and actually zero. Moreover, while knobs are sometimes seen on virus-like particles as they exit a cell, they disappear within a day or so, and the particles therefore cannot be infectious. Some researchers have suggested that the spikes are an artefact produced by the heavy-metal stain used in electron microscopy (Perth Group, 2011; Papadopulos et al., 2017, p. 62).
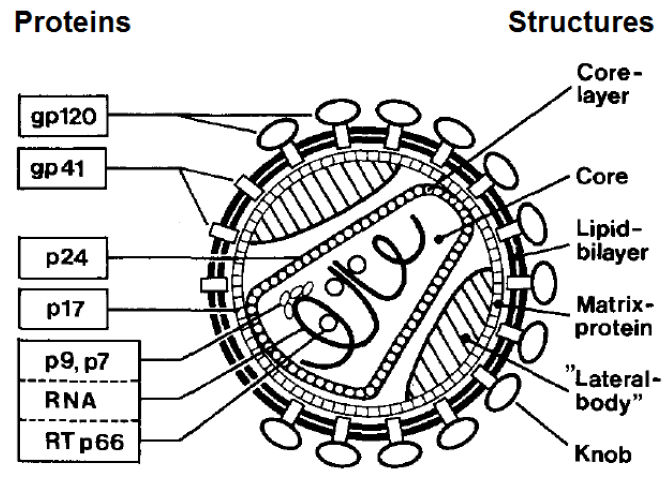
Hans Gelderblom’s model of the ‘ideal’ HIV particle. (Papadopulos et al., 2017, p. 11)

Computer-generated image of what ‘HIV’ might look like if it really existed.
The experiments by Bess et al. detected only three of the 15 proteins that allegedly compose HIV: p6/7, p17 and p24. However, they are more likely to be cellular proteins since they were found not only in the material supposedly containing ‘HIV’ but also in the ‘uninfected’ material, though in lower quantities (see below).
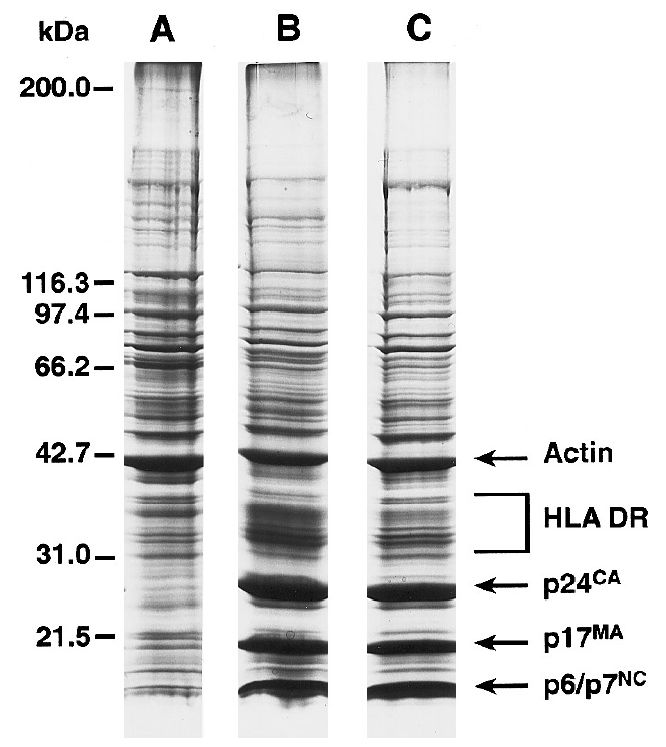
Protein profiles for 1.16 g/ml material from an ‘uninfected’ cell culture (A) and from ‘HIV-infected’ cell cultures (B and C). Actin and HLA DR = cellular proteins; kDa = molecular weight scale. (Bess et al., 1997)
The Perth Group concludes that the experiments by Montagnier, Gallo, Gluschankof and Bess failed to purify and prove the existence of ‘HIV’ particles and failed to prove the existence of ‘HIV’ proteins and RNA. If there are no ‘HIV’ proteins, there can be no ‘HIV’ genome. To define the genome of a retrovirus, the RNA must be extracted from purified retroviral particles and then sequenced, but no researcher has ever determined the ‘HIV’ genome in this manner.
Based on the genetic fragments found in patients’ blood, AIDS scientists estimate that 100 million or more genetically distinct variants of HIV are present in any AIDS patient, due to its extraordinary ability to mutate. HIV genomes are said to vary by between 3% and 40%, whereas in other alleged RNA viruses variations greater than 1% are considered ‘extreme’. There is not a single study proving the existence of the ‘HIV’ genome in even one cell of a single AIDS patient. All ‘HIV’ genetic sequences are obtained from artificially stimulated, immortalized cell cultures (often cancer cells) containing all sorts of contaminants.
The Perth Group argues that much of the genetic material attributed to HIV is in fact DNA or RNA from stressed or dying cells, which are known to produce retroviral-like particles. In other words, we are looking at chaotic genetic activity from within disordered cells rather than a unique, invasive viral entity. In their view, ‘HIV’ is simply ‘a metaphor for a lot of quasi-related phenomena’, and a consequence of challenged health rather than its cause.
Great efforts have been made to prove the HIV theory of AIDS by administering material taken from AIDS patients (assumed to contain the virus) to monkeys and ‘humanized mice’ (i.e. mice engineered to carry human genes, cells, tissues and/or organs), but none of the animals developed AIDS (Perth Group, 2016b).
To maintain the AIDS scare, frequent use is made of alarmist estimates and projections. For instance, the 1999 United Nations AIDS Report estimated that 2.5 million people throughout the world died of AIDS in 1998. Yet the November 1999 WHO Weekly Epidemiological Record reported that only 2.2 million people worldwide had ever received a diagnosis of AIDS – and this included many people who remained alive and well (Maggiore, 2000, p. 14). The UN estimate received wide publicity while the actual WHO case count was neglected.
According to UNAIDS, by 2023 the total number of worldwide AIDS fatalities since the alleged epidemic began was 42.3 million, and the total number of people ever ‘infected with HIV’ was 88.4 million. Publicizing cumulative totals such as these makes it possible to cite ever-growing numbers even though ‘AIDS’ is declining. HIV/AIDS was listed as the 16th leading cause of death worldwide in 2021.
In 1986 it was predicted that 3 to 5 million Americans would be HIV-positive and 1 million would have died from AIDS by 1996 (Maggiore, 2000, p. 14). However, since the 1980s the total number of HIV-positive people in the United States has been around 0.4% of the population, or approximately 1 million people. In 2022 the estimate was 1.2 million, of whom 13% are said to be unaware that they are HIV-positive.
In 1995, the death rate from ‘HIV’ in the United States peaked at 16.2 per 100,000 people. By 2022, the number had fallen to 1.3 per 100,000; there were 19,310 deaths among HIV-positive adults and adolescents. In the US anyone with an AIDS diagnosis who dies is classed as an AIDS death, even if they die from accidents, non-AIDS illnesses, drug side effects, etc. Gay and bisexual men account for 71% of new HIV diagnoses in the United States. HIV/AIDS is now the 47th leading cause of death in the US. The biggest killer is officially said to be heart disease, but Peter Gøtzsche argues that it is really prescription drugs, which cause an estimated 882,000 deaths per year. The National Institutes of Health spends nearly 20 times more on HIV/AIDS, per death, than on any other significant medical or public health concern (Shenton, 2015, p. xviii).
In 1985 the United Kingdom’s Royal College of Nursing predicted that 1 million people in Britain would have AIDS by 1991 unless the killer disease was brought under control. However, in 1991 there were 20,403 people ‘living with HIV’ in the UK, and 523 HIV deaths. The figures for 2021 are 128,121 ‘infected’ people and 247 deaths. In 2020, 49% of new HIV diagnoses in England were in heterosexuals, compared with 45% in gay and bisexual men. However, gay and bisexual men are still far more impacted by HIV relative to population size.
In the United States, AIDS cases increased from 1981 to 1992 and then declined, whereas alleged HIV infections remained more or less constant – indicating that ‘HIV’ was not the cause of the AIDS epidemics of the early 1980s. The failure of AIDS to progress exponentially shows that it is not a contagious disease caused by an infectious virus. Instead it has acted like lifestyle diseases, such as lung cancer from smoking. If contagious, it would also have spread randomly through the population. Instead it is highly nonrandom with regard to sex (80% of patients are male), sexual persuasion (over 60% are homosexual), and age (85% are aged 25-49) (Bialy, 2004, p. 186). In the West, AIDS is still largely confined to its two original risk groups: promiscuous gay men account for about two-thirds of the cases, and drug addicts for most of the rest.
In the United States, AIDS was first noted around 1980 in New York, Los Angeles and San Francisco; HIV is alleged to have arrived in those communities about 10 years earlier. Tests for HIV have been widely carried out since 1985, and straight away HIV-positive people were found in every sector of society and in every part of the US. It is highly unlikely that HIV could have spread so rapidly into the general population across the country. For a start, the geographic distribution of HIV does not look like a spread from the AIDS epicentres; HIV has always been more prevalent in the east and south of the US than in the west, and is least prevalent in northern and central parts. The conventional view of HIV/AIDS is unable to explain this asymmetry, for ‘one would hardly expect a sexually transmitted infection to display so unvarying a geographic distribution’ (Bauer, 2005, p. 582).
‘HIV’ is supposedly sexually transmitted, but this has never been proved by isolating HIV from genital secretions of index cases followed by tracing and testing of sexual contacts. Padian et al. (1996) carried out a 10-year study of heterosexual couples where one partner was HIV-positive and the other was HIV-negative, and concluded that ‘infectivity for male-to-female transmission’ is only 0.0009 per contact and ‘infectivity for female-to-male transmission’ is about eight times lower; the main risk factors were injection drug use, anal sex, and a history of sexually transmitted diseases. In other words, only about 1 in 1000 unprotected sexual contacts ‘transmits HIV’. Bialy (2004, p. 209) noted that since only around 1 in 275 US citizens is HIV-infected, an average uninfected citizen would need 275,000 random sexual contacts to get infected and spread HIV – an unlikely basis for an epidemic!
Prostitutes commonly become infected with syphilis, gonorrhoea and herpes, but rarely become infected with ‘HIV’, unless they abuse intravenous drugs. Likewise, the wives or husbands of haemophiliacs don’t commonly get AIDS. The CDC admits that ‘HIV transmission’ in healthcare settings is ‘extremely rare’. By 2001 there were 57 possible cases of medical workers contracting AIDS from patients, i.e. three per year, but this could be because a variety of not necessarily serious health challenges can cause people to test positive (Bauer, 2007, p. 198). In other words, the evidence shows that ‘HIV’ is extremely difficult to ‘transmit’ to a healthy individual. If HIV is not a real virus, there is obviously nothing to transmit.
Further evidence that ‘HIV’ is not sexually transmitted is provided by comparisons of the incidence of AIDS in different population groups and the variation of ‘infection’ rate with age (Bauer, 2006a). Newborn babies test HIV-positive about four times more often than children from about one year of age to the pre-teen years, and about 10 times more often than children in their early teens. From the teens on, the ‘infection’ rate in all studied groups follows the same course, increasing into the middle adult years and then declining again towards old age, more so for men than for women. Psychiatric patients test ‘HIV-positive’ significantly more often than people attending clinics for sexually transmitted diseases, or clinics providing HIV tests and counselling. The prevalence of HIV is much higher in critically ill emergency-room patients than in the least ill patients, and among tuberculosis patients it is about the same as or slightly higher than among those visiting STD clinics.
The frequency of positive HIV tests also correlates with racial category (Bauer, 2006b, 2024). In every occupational, social or other group tested in the US, at all ages and for both sexes, the prevalence of HIV increases in the order: Asian – white – Native American – Hispanic – black. Data from South Africa display a similar sequence: white/Asian-Indian – coloured – black. Almost all countries where over 1% of the population test HIV-positive are in southern Africa. In the United States and United Kingdom, black people are about 10 times more likely to test positive than other racial groups, and 50 times more likely to do so in South Africa. The only explanation under the current paradigm is that blacks are more prone to risky, promiscuous, sexual behaviour and sharing of infected needles for injecting illegal drugs than whites, Asians or Native Americans. But surveys of actual behaviour contradict this.
HIV tests are nonspecific and clearly do not track a sexually transmitted agent. Testing HIV-positive is an indicator of challenged health or actual illness, and the intensity of the body’s response to health challenges can perhaps be modified by genes associated with the immune system, which differ for different racial groups. The tests that supposedly detect antibodies specific to HIV are actually detecting signs of some sort of physiological stress. The fact that newborn babies test positive more frequently than older children shows that ‘HIV-positive’ is not necessarily a permanent condition.
AIDS propagandists like to claim that Africa is being ravaged by an HIV/AIDS epidemic. Nowadays HIV/AIDS is said to cause an average of 1.1% of deaths worldwide, but in southern Africa the figure can be as high as 13.5%. In Zimbabwe it allegedly caused 54.4% of deaths in 1997, but the figure had fallen to 10.4% by 2021 (ourworldindata). According to UNAIDS, in 2023 there were 25.9 million people ‘living with HIV’ in Sub-Saharan Africa, and 390,000 AIDS-related deaths. However, as Christine Maggiore puts it, ‘Unfounded estimates, rather than unprotected sex, are responsible for the alarming number of AIDS cases said to occur in Africa’ (2000, p. 20).
Under the WHO’s Bangui definition, Africans are diagnosed with AIDS without an HIV test if they score at least 12 points based on a list of symptoms which includes: over 10% weight loss (4 points), protracted weakness (4), prolonged fevers for a month or more (3), prolonged diarrhoea (3), thrush (4), persistent cutaneous herpes (4), shingles (4), persistent itching (4), and a cough (2). These same symptoms are caused by conditions that run rampant in Africa, such as malaria, tuberculosis, parasitic infections, malnutrition, and unsanitary drinking and bathing water. Since long-standing problems such as poverty and poor sanitation affect both sexes equally, AIDS in Africa also affects both sexes fairly equally. In 2023, women and girls accounted for 62% of all new ‘HIV infections’ in sub-Saharan Africa.
Several large studies have found that among thousands of randomly selected Africans with standard AIDS diseases, fewer than half were HIV-positive (Duesberg, 1996, p. 295). South Africa is the only sub-Saharan country in which an HIV antibody test is required before labelling an otherwise common disease or combination of diseases ‘AIDS’. But as already noted, positive results in HIV tests can be produced by exposure to diseases that are widespread in Africa.
Pregnant African women are routinely tested for syphilis at antenatal clinics, and some of the blood samples left behind are anonymously given a single ELISA antibody test. The results are then extrapolated to the general population via computer simulations. However, pregnancy is a known source of ‘false positives’ (Culshaw, 2007, pp. 85-6).
A 1998 news report, based on UN estimates, claimed that ‘a Kenyan dies of AIDS every 3 minutes’. If that were true, 175,000 Kenyans would die of AIDS every year – yet the total number of diagnosed AIDS cases in that country from 1981 to 1999 was less than half this figure (81,492) and many of these people were still alive and well (Maggiore, 2000, pp. 19-20). In 1987 the WHO estimated that there were one million cases of ‘HIV disease’ in Uganda. Yet 10 years later the cumulative number of AIDS cases actually reported was 55,000. ‘Nobody knew what had happened to the other 945,000,’ says James Hogan dryly (2004, p. 322).
In 1996 WHO statisticians multiplied reported AIDS cases in Africa by 12 to reach estimated totals; in 1997, by 17; and over an 18-month period in 1997/98, by 47. One study claimed that young adults with HIV in Africa were 87 times more likely to die prematurely than their uninfected contemporaries. But newspaper reports forgot to mention that this was an extrapolation based on just 14 deaths and five actual AIDS diagnoses (Hodgkinson, 2003).
In 2000, 5000 scientists signed the Durban Declaration, which predicted that 24 million HIV-positive Africans would die within five years. In 2008, AIDS ‘experts’ estimated that between 2000 and 2005 300,000 people in South Africa had died from HIV every year. However, Peter Duesberg et al. (2011) found that South Africa attributed only about 10,000 deaths per year to HIV over that period and its population had increased at a steady rate of 500,000 per year, even though 25% to 30% were ‘HIV-positive’.
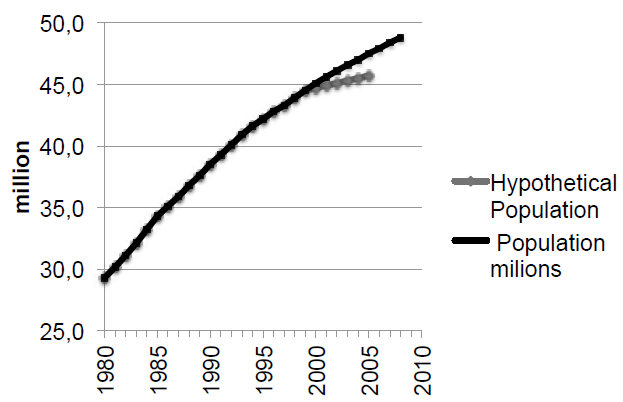
The population growth curve of South Africa from 1980 to 2007, showing the hypothetical lower growth that would have occurred from 2000 to 2005 if an AIDS epidemic had really claimed 300,000 lives per year.
From 1980 to 2008 Uganda’s population increased from 12 to 31 million, and that of Sub-Saharan Africa as a whole doubled from 400 to 800 million, despite claims of devastating AIDS epidemics. The steady growth of the African population was clearly unaffected by the rise of ‘HIV’ prevalence from 0.7% to 30% between 1990 and 2000. As Duesberg et al. (2011) say, the real reason for the sharp increase in HIV prevalence was the ‘new epidemic of HIV-antibody testing’. Wildly inaccurate predictions of a rampaging AIDS epidemic have also been made about Brazil, India, Thailand and other tropical places with endemic public health problems and poor health statistics.
Based on the conventional view of HIV/AIDS, every African not known to be a homosexual or drug abuser is presumed to have acquired AIDS through heterosexual intercourse – thereby resurrecting the racist tendency to stereotype Africans as hypersexual. Lecturing people on their morals, distributing condoms, and poisoning African babies with ‘anti-AIDS’ drugs will do nothing to solve the root causes of Africa’s health problems.
More insidious, funds and resources are withdrawn from the support of low-cost but effective traditional clinics and the provision of basic nutrition, clean drinking water, and sanitation, and directed instead to ruinously expensive programs to contain a virus that exists for the most part in WHO statisticians’ computers. (Hogan, 2004, p. 323)
Many Africans participate in perpetuating the myth of an AIDS epidemic in Africa. The huge international funds poured into AIDS and HIV work mean that politicians and health workers have a strong incentive to reclassify as AIDS old diseases that have always been endemic in tropical Africa. When African doctors are sent to AIDS conferences around the world, the daily allowance they receive can be equal to what they earn in a whole year at home.
It has become a joke in Uganda that you are not allowed to die of anything but AIDS. If someone is run over by a truck, doctors have been known to attribute it to AIDS-related suicide (Hogan, 2004). The Ugandan government could afford to spend less than $1 a head on healthcare from its own funds, but in just one year it received $6 million for AIDS research and prevention from foreign agencies. As one commentator puts it, dysentery and malaria do not inspire headlines or fatten public health budgets; infectious ‘plagues’ do (Hodgkinson, 2003). What’s more, people in developing countries can obtain help from agencies if they have lost family members to ‘AIDS’ – but not if the deaths are attributed to other causes.
There is thus a vast overdiagnosis of AIDS and ‘HIV disease’ in Africa and other countries where malnutrition, impoverished living conditions and the associated diseases are the real killers. The WHO rightly calls extreme poverty ‘the world’s biggest killer and the greatest cause of ill-health and suffering across the globe’.
The HIV/AIDS scare gave a tremendous boost to the pharmaceutical industry, which has reaped enormous profits by peddling highly toxic antiretroviral drugs (ARVs). The main impact of these drugs, however, has not been to improve patients’ long-term health, but to boost the number of ‘AIDS’ cases and deaths. In 2023 an estimated 30.7 million people worldwide were on antiretroviral drugs, and the top 10 drugs generated $25.75 billion in sales. HIV care in the United States costs an average of $25,000-$30,000 per patient per year, of which 67%-70% is spent on ARVs.
AZT (azidothymidine) is a highly toxic chemical compound originally created for use as a cancer treatment. It is known as a nucleoside analogue drug, or DNA chain terminator, meaning that it stops DNA from replicating. It therefore destroys all growing cells, including new cells produced in bone marrow, where the immune system is generated. In 1964, experiments with AZT on mice with cancer showed that it was so effective in destroying healthy growing cells that the mice died of extreme toxicity. As a result, the drug was shelved and no patent was ever filed.
20 years later the pharmaceutical company Burroughs Wellcome (now GlaxoSmithKline) launched a campaign to remarket AZT (also known as zidovudine and Retrovir) as an anti-HIV drug. In 1987, the US Food and Drug Administration (FDA) gave its approval after abbreviated trials of less than six months sponsored by the drug’s manufacturer, who selected for publication only those trials with seemingly favourable outcomes. AZT is much more toxic than recreational drugs such as cocaine and heroin, and is now widely understood to have been prescribed in overly large doses. In the early days, no one lived more than a few years on AZT treatment. Its victims include celebrities such as Rock Hudson, Arthur Ashe and Freddie Mercury.

Laboratories receive AZT in bottles carrying this special label. The skull-and-crossbones on a bright orange background signifies an unusual chemical hazard. The label appears on bottles containing as little as 25 milligrams, a small fraction (1/20 to 1/60) of the daily dose of 500 to 1500 mg that AIDS patients used to be prescribed.
In 1994 the ability of AZT to delay the progression to AIDS was investigated by the British-French Concorde study, the largest placebo-controlled study of its kind. It investigated 1749 HIV-positive subjects and found that AZT is unable to prevent AIDS and increases mortality by 25% (Duesberg et al., 2003, p. 399). In addition to destroying T-cells, B-cells and the red blood cells that carry oxygen throughout the body, AZT and similar drugs – e.g. Epivir (3TC), Zerit (D4T), Hivid (ddC) and Videx (ddI) – destroy the kidneys, liver, intestines, muscle tissue and the central nervous system. From 1988 to 1996, AZT caused over 96% of the 235,000 AIDS deaths in the United States, with 140,000 of the victims being HIV-positive young gay men (Miller, 2015). Gay activist organizations earned large sums of money by advertizing the ‘benefits’ of AZT. They enthusiastically supported the virus hypothesis because it diverted attention away from lifestyle factors.

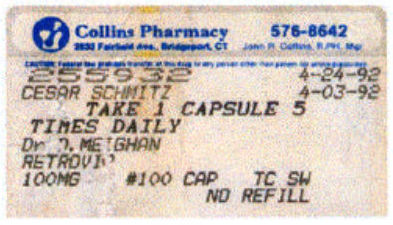
In 1992 Cesar Schmitz was healthy but tested HIV-positive. After starting AZT, he suffered from nausea, diarrhoea and weight loss. In 1994 he stopped AZT and his symptoms disappeared. But in 1998 he developed lymphoma (lymph cancer) and died. People who take AZT for three years have a 46% chance of developing lymphoma. (lewrockwell.com)
In 1996 a new class of antiviral drugs was introduced, known as protease inhibitors, which are used in combination with older chemotherapy compounds such as AZT. The mixture of these treatments is called a ‘combination cocktail’ or ‘highly active antiretroviral therapy’ (HAART). They were licensed in the US through a fast-track procedure, after the trials were prematurely terminated (Shenton, 2015, pp. 215-6). As with AZT, the media was full of hype about their ‘miraculous’ effects, though their manufacturers admit the drugs cannot cure AIDS.
Well-documented side effects include nausea and vomiting, diarrhoea, headache, muscle and joint pain, severe fatigue, loss of appetite, sexual dysfunction, fever, chills, skin rashes, dizziness, abdominal pain, depression, sleep disorders, arthritis, dementia, cancer, heart disease, kidney disease, bone disease, diabetes, liver failure, physical deformities (inculding hunchbacks), pancreatitis, nervous system damage, and a hypersensitivity reaction that can result in sudden death. The drugs have a failure rate of 50%, and as many as 40% of participants dropped out of protease inhibitor drug trials due to adverse effects (Maggiore, 2000, p. 22; Bauer, 2017).
Even the US National Institutes of Health has admitted that ‘a growing proportion of patients receiving long-term antiretroviral therapy are experiencing treatment failure, drug toxicities, side effects, and drug resistance. In this regard, recent studies have noted an increased incidence of malignancies, cardiovascular and metabolic complications, and premature aging associated with long-term HIV disease or antiretroviral therapy’ (Fauci & Whitescarver, 2011). There is evidence that antiretroviral drugs cause mitochondrial mutations that accelerate the aging of cells, leading to multi-organ disease (Payne et al., 2011).
The drugs were praised because patients’ ‘viral load’ decreased and their CD4 T-cell counts increased. But at the same time many patients became sicker. So a new medical condition was invented, known as ‘immune reconstitution syndrome’, in which AIDS-like illnesses are said to be caused, in some mysterious manner, by the recovering immune system. However, it was impossible to deny the ‘unexpected toxicities’ of the drugs, and in 2001 the US government reversed its policy of ‘hit hard, hit early’ for HIV-positive people, and recommended instead that antiretroviral treatment should be delayed as long as possible for those with no symptoms of illness. Drug manufacturers were also ordered to tone down their upbeat ads for AIDS medications, and some drugs were withdrawn.
HAART is not said to destroy ‘HIV’, but to interrupt its replication cycle. Since none of the drugs has any effect on the transcription of ‘HIV’ DNA into ‘HIV’ RNA, a decrease in the latter, i.e. the ‘viral load’, should always be preceded by a decrease in the former, but this is not the case. This suggests that ‘HIV’ RNA is not related to an invasive retrovirus, but is a modified or new form of cellular RNA. Since antiretroviral drugs are oxidizing agents, they will modify a person’s genetic material and reduce the likelihood that they will have genetic sequences that match the ‘primers’ used in PCR tests, because the primers are derived from cell cultures that have not been exposed to the extra stress of these drugs. As a result, patients’ ‘viral load’ will appear to decrease or even become undetectable (Papadopulos et al., 2017).
HIV-positive people who are very sick may experience some benefit after starting antiretroviral therapy. Later, however, the drugs tend to lose their effectiveness, which is taken to mean that ‘HIV’ becomes resistant. However, the temporary reprieve does not have anything to do with the drugs’ effect on any virus. Antiretroviral drugs are toxic to all living things and consequently have antimicrobial properties; they can therefore suppress the symptoms of the microbial diseases that affect most AIDS patients. Another potential factor is hormesis: as with low doses of radiation, drug treatment may initially stimulate the immune system to work harder. And finally there is the placebo effect: belief in the efficacy of a ‘life-saving’ drug might for a time override its adverse effects (see Mass psychosis).
Although the protease inhibitor ‘combo cocktails’ are often claimed to be behind
the decline in AIDS, the decline began several years before these drugs became available for
general use. A more likely explanation for the lower death rate is that since the 1993 revision of the
AIDS definition in the United States, more than half of all newly diagnosed AIDS cases involve HIV-positive people with no
symptoms of illness; by 1997 the figure stood at 65%. Another important factor is that dosages of nucleoside analogue drugs and protease inhibitors are now much lower than the massive doses of AZT that used to be prescribed. In the late 1980s, some patients had to take 400 mg of AZT every four hours, day and night. In the HAART era the recommended dose of AZT is 300 mg twice daily, i.e. a 75% reduction from 2.4 g to 0.6 g (Papadopulos et al., 2017, p. 82).

The CDC’s own data show that AIDS deaths began to decline at the end of 1995, before the release of new ‘wonder drugs’, and that AIDS cases began to decline before that. They would both have started to decline earlier if the CDC hadn’t expanded the definition of AIDS in 1993. Only 19% of HIV-positive people were actually on the new drugs by mid-1996.
The immune suppression supposedly caused by HIV is therefore being tackled with drugs that are themselves notoriously immunosuppressive, and cause AIDS-defining conditions such as diarrhoea, dementia, lymphoma, muscle wasting, and T-cell depletion. These medications amount to ‘AIDS by prescription’ – but patients are told they must take them or die. This is the real tragedy of the HIV/AIDS scandal: hundreds of thousands of people – many of whom are initially perfectly healthy – have been and are still being poisoned with dangerous, health-destroying drugs. Patients are required to pop up to 30 pills a day and are warned that if they fail to adhere to the dosages and schedule, their virus will mutate into new drug-resistant strains. Patients who quit the drugs due to the intolerable side effects have been told that they are ‘in denial’ and depicted as a public health menace.
Even babies and infants are not spared. Pregnant mothers who test HIV-positive have been advised to abort or take AZT, despite its horrible side effects. One study found birth defects in 10% of babies born to women who took AZT during pregnancy. A major Italian survey showed that children born to mothers treated with AZT in pregnancy were more likely to get severely sick and die by the age of three than those whose mothers were left untreated (Hodgkinson, 2007).
Several US states require mandatory HIV antibody testing for newborns in public hospitals (nytimes). Healthy babies who test HIV-positive are usually treated with antiretroviral drugs, sometimes against the wishes of parents; parents who refuse to cooperate have been threatened with prosecution for child neglect. Even on the standard view of HIV/AIDS, such treatment would be unwarranted as 50-75% of ‘HIV’ infection in newborns represents antibodies transferred from the mother. Moreover, 75% of HIV-positive babies revert to HIV-negative without medical intervention, and 90% of babies born to healthy HIV-positive mothers test negative without drug therapy (Bauer, 2006b). Mothering magazine has carried articles warning pregnant women not to use antiviral drugs during pregnancy and containing heartbreaking accounts of the clinical consequences for the babies, and of the pressures placed on mothers to administer poisonous drugs to their babies.
Trials of ‘anti-AIDS’ drugs, from AZT onwards, have commonly been conducted without proper controls; ideally, a drug should be tested by giving half the subjects the real drug and the other half a fake drug (placebo), and the trial should be double-blind, meaning that neither the subjects nor the experimenters know which subjects are in the test or control group – but this standard scientific practice has often been discarded. Those who criticize such lax practices or question the safety and efficacy of the allegedly ‘life-saving’ drugs have been labelled ‘refuseniks’, ‘denialists’ and even ‘murderers’ by pharmaceutical representatives, AIDS activists and lap-dog journalists.
Christine Maggiore (2000, p. 43) writes: ‘Surprisingly, it is not considered a conflict of interest when AIDS researchers own stock in the companies whose products they test, or when they are hired to run the drug trials they publish in medical journals. It is common practice for drug companies to pay researchers to author favorable articles about their products.’ As former pharmaceutical drug developer David Rasnick says, ‘The scientific-medical complex is a $2 trillion industry. You can buy a tremendous amount of consensus for that kind of money. ... Science has totally capitulated to corporate interests’ (Farber, 2006).
AIDS researchers claim that anti-HIV drug cocktails reduce morbidity and mortality, based on surveys that investigated how long clinically healthy HIV-positive people survived on various drugs. Yet none of the surveys included an untreated control group to see whether the healthy subjects would have survived anyway. The disclaimers enclosed by manufacturers with all anti-HIV medications indicate that none of them has been shown to prolong life, and that all of them cause debilitating side effects, some of which are indistinguishable from the symptoms of AIDS. In short, there are no clinical trials showing that people taking anti-HIV drugs live longer or at least better lives than HIV-positive people not taking the drugs.
However, Duesberg et al. (2003) cite around 50 studies showing that HIV-positive people treated with antiretroviral medications experience AIDS-defining illnesses at a greater rate than untreated HIV-positive control subjects; the drugs increase the mortality of HIV-positive individuals four- to six-fold. A study of 36 German AIDS patients who volunteered to abstain from anti-HIV treatment began in 1985. Only 8% had since died, compared with 63% of German AIDS patients as a whole, most of whom had been treated with antiretroviral drugs since 1987.
The leading cause of death among medicated ‘HIV-positive’ people is not even an AIDS-defining disease, but liver failure, a well-documented adverse effect of protease inhibitors (Culshaw, 2007, p. 29). A further 25-35% of deaths are due to cancer, which no one has ever claimed to be caused by HIV (Shenton, 2015, p. lxiii). When HIV-positive individuals using antiretroviral drugs die, no autopsies are carried out to determine whether their death was caused by the drugs.
The WHO estimated that in 2000 there were 34.3 million HIV-positive people worldwide and 407,000 AIDS cases. Even if it were assumed that all AIDS cases were fatal in a given year, which is hardly likely, the corresponding mortality rate would be only 1.4%. By contrast, the mortality rate of HIV-positive people receiving antiretroviral medications in the US and Canada was found to be between 6.7% and 8.8% (Duesberg et al., 2003). As Henry Bauer (2007, p. 241) comments: ‘Something is very wrong if the worldwide mortality rate of largely untreated HIV-positive people in under-developed countries is only about one-fifth or one-sixth of the mortality of HIV-positive people being given the best available antiretroviral medications in the world’s most developed countries.’
The massive injection of funds into HIV/AIDS has created an army of HIV-AIDS ‘experts’ – scientists, journalists and activists – who cannot afford to question the direction of their crusade as it would threaten their livelihood.
In 2000 the South African President Thabo Mbeki attempted to start a dialogue between orthodox and dissident AIDS scientists in the run-up to the international AIDS conference in Durban. However, mainstream scientists refused to participate. Instead, 5000 scientists signed a declaration (published in Nature on 6 July 2000), proclaiming the ‘true gospel’ that AIDS is caused by HIV, and accusing dissenting scientists of threatening ‘countless lives’. A point-by-point refutation of the Durban Declaration was published (Johnston et al., 2001), but was ignored.
Harvey Bialy, an opponent of official HIV/AIDS theory, once challenged a prominent AIDS expert to a debate, but the latter replied by saying: ‘The science community does not “debate” with the AIDS denialists, it treats them with the utter contempt that they deserve and exposes them for the charlatans that they are’ (Culshaw, 2007, p. 68). The fact that HIV=AIDS proponents prefer to denounce their opponents rather than engage in serious debate is very revealing. As James Hogan says, repressing dissenting views ‘is not the way of science, but of a fanatical religion putting down heresy’ (2004, p. 329).
Christine Maggiore writes:
we have constructed a powerful AIDS establishment that regulates our news, limits our access to information, and demands an ever greater allocation of our resources and support. Rather than helping to resolve AIDS, we have funded the growth of multi-billion dollar industries, institutions and organizations that depend on AIDS and on our continued devotion to the narrow and unproductive HIV hypothesis. (2000, p. 61)
Nicholas Regush, a medical science reporter, comments:
Beware the scientist who believes that mainstream research thinking on any public health issue is equivalent to truth. Or the scientist who bullies or ridicules other scientists because they oppose the prevailing view. This is a person who has become what I would call a propagandist and should not be trusted. ... In all the time I’ve worked as a journalist, I’ve never come across a nastier group of people to interview than those propagandists who work in HIV research. (Maggiore, 2000, p. 63)
David Rasnick remarks:
As a scientist who has studied AIDS for 16 years, I have determined that AIDS has little to do with science and is not even primarily a medical issue. AIDS is a sociological phenomenon held together by fear, creating a kind of medical McCarthyism that has transgressed and collapsed all the rules of science, and has imposed a brew of belief and pseudoscience on a vulnerable public. (Maggiore, 2000, p. 63)
John Lauritsen (2007), a gay activist who opposed the virus theory, describes HIV/AIDS as ‘the greatest blunder and the greatest hoax in medical history – an epidemic of incompetence and an epidemic of lies’. He adds: ‘As AIDS became a religion, a death cult – with sacred commodities, dogmas, rituals and sacrifices – any expression of scepticism was tantamount to blasphemy.’
Kary Mullis stated:
In the AIDS field, there is a widespread neurosis among scientists, but the frenzy with which people approach the HIV debate has slacked off, because there’s just so much slowly accumulating evidence against them. It’s really hard for them to deal with it. They made a really big mistake and they’re not ever going to fix it. They’re still poisoning people. (Farber, 2006)
As Mullis puts it: ‘We know that to err is human, but the HIV/AIDS hypothesis is one hell of a mistake’ (Duesberg, 1996, p. xiv).
Blaming noninfectious diseases on infectious microbes has occurred many times before. For example, scurvy, pellagra, SMON and beriberi were each in turn blamed on mysterious infectious agents, sometimes leading to control measures that only made things worse. Scurvy turned out to be caused by vitamin C deficiency, pellagra by niacin deficiency, and beriberi by vitamin B1 deficiency.
The SMON epidemic struck Japan in 1950s and 60s, and was eventually found to be caused by a drug called clioquinol, which doctors had prescribed to treat early symptoms of SMON itself (e.g. diarrhoea). SMON cases rose and fell with sales of clioquinol, and disappeared after it was banned. But by the time the virus-hunters realized their blunder, thousands had died and many victims were left blind or paralyzed. Nowadays, the virus-hunting establishment prefers to keep quiet about this embarrassing ‘incident’.
Peter Duesberg, a virologist and leading AIDS dissident, says that while the war on SMON was a ‘molehill of misdirected science’, AIDS is ‘an unmovable mountain’. SMON and AIDS, he says, ‘have become episodes in a long series of miscalculations emanating from a single ongoing, self-propagating scientific program – microbe hunting’ (1996, p. 29). Virus hunting was nearly discredited by the failed war on cancer, but enjoyed a spectacular revival with the HIV=AIDS hypothesis.
Several scientists have argued that HIV alone is not sufficient to cause AIDS. Montagnier has repeatedly stated this, and Gallo has also hinted at it, though current orthodox opinion still resists this view. To explain how ‘HIV’ supposedly kills at least 10,000 times more T-cells than it actively infects, it has been suggested that it acts in conjunction with various ‘cofactors’, which may include microbes, ulcers, stress and diet.
Although Duesberg believes that HIV is a genuine, invasive retrovirus, he objects that since it is extremely rare and dormant in most antibody-positive AIDS patients, it is hard to imagine how it could contribute to the various AIDS ‘cofactors’. Claims that HIV depends on ‘clinical illness promotion factors’ or on a ‘preexisting immune abnormality’ are, he says, ‘euphemisms for saying that HIV cannot cause AIDS until something else does’ (1996, p. 551). He argues that, far from being the ferocious cell-killer portrayed by the media, HIV is a harmless ‘passenger virus’. He believes that the real causes of the destruction of the immune system are drug abuse, heavy exposure to blood and blood products, and toxic medical treatments directed against HIV.
For putting forward these views, Duesberg has been pilloried and ostracized by the scientific establishment since 1987. He has been labelled a scientific psychopath who should be imprisoned, and accused of having the blood of African AIDS babies on his hands. Federal support for his laboratory was cut off so that by the end of the 1980s he couldn’t afford a secretary. He had to fight for even routine pay increases from the University of California at Berkeley. Graduate students were advised to shun his classes or risk adverse consequences to their careers. To humiliate him further, he was placed in charge of his university’s annual picnic committee.
Duesberg had previously received ongoing funding as a recipient of the NIH’s prestigious Outstanding Investigator Award, but after challenging the HIV hypothesis, he had 25 research grant applications rejected. Publication in the mainstream scientific literature was denied, including the right of reply to personal attacks carried in Nature. He ceased to be invited to scientific conferences, and colleagues even declared that they would refuse to attend any conference that included him. The claim is often made that Duesberg has been discredited, yet ‘there is no record of this “discrediting” anywhere in the scientific literature’ (Culshaw, 2007, p. 13).
In 2009, Duesberg and his coauthors submitted a paper to the journal Medical Hypotheses, criticizing a Harvard study which estimated that 330,000 people per year died of AIDs in South Africa in the period 2000-2005 and arguing that a more realistic figure was 12,000 per year. The HIV/AIDS establishment went on the attack and forced the journal’s publisher, Elsevier, to withdraw the article, on the grounds that it might damage global public health. Elsevier fired the editor and stopped publishing the journal for several months until it could find a more docile replacement.
Anthony Fauci, former director of the National Institute of Allergy and Infectious Diseases (NIAID), acted as the United States’ AIDS tsar for over 30 years, and later as its Covid tsar. His unethical role in furthering the agenda of big pharma and suppressing scientific dissent has been thoroughly documented by Robert F. Kennedy (2021). On one occasion, Duesberg was flown to New York to appear on Good Morning America, but Fauci put a stop to this and appeared on the show in his place (Miller, 2015).
As already stated, the Perth Group of scientists argues that ‘HIV’ does not exist. Beginning in 1983, it proposed an alternative theory of AIDS that highlights the key role of oxidative stress in undermining our health. Oxidation means the loss of electrons, while reduction means the gaining of electrons. Examples of oxidation include the rotting of food, rusting of metal, burning of fuels, and ageing. Oxidants disrupt cellular equilibrium, and can cause diseases such as cancer and cardiovascular disorders.
The cellular oxidation theory predicted that the tissues of AIDS patients and those at risk would be oxidized, and this was quickly confirmed. AIDS risk groups are exposed to a variety of oxidative agents, including semen, nitrites, recreational drugs, Factor VIII (a blood-clotting agent used by haemophiliacs), ‘infectious’ microbes, and antiretroviral drugs. Poverty, malnutrition and poor sanitation can also result in biological oxidation, and these are the main factors behind ‘AIDS’ diseases in Africa. The effectiveness of using antioxidants to prevent and treat AIDS has been confirmed by a placebo-controlled trial (Perth Group, 2016a).
As far as ‘microbial infections’ (e.g. pneumonia and tuberculosis) are concerned, the Perth Group emphasizes that the underlying problem is not the microbes themselves, which do not attack healthy cells, but a compromised bioterrain. This results in the proliferation of bacteria etc., which feed on dead and decaying tissue and can produce toxins while doing so. Exposure to oxidizing agents occurs long before patients develop such infections. Orthodox medicine recognizes that microbes found in people with certain diseases are also found in perfectly healthy individuals. It coined the term ‘opportunistic infections’ to describe such conditions, arguing that the microbes in question only become ‘pathogenic’ when the body’s defence system is impaired.
Perth Group scientists have faced relentless censorship and attacks by those who benefit from perpetuation of the HIV=AIDS myth. They argue that the existence of HIV is fatally undermined by the following facts:
(1) heroic attempts to isolate such a virus always fail, despite huge financial incentives and numerous attempts to do so by an enormous army of scientists dedicated to ‘HIV’ ...; (2) what is called HIV RNA and DNA comes in many sizes and varieties that always differ from each other (no two are alike, even when abstracted from the same patient), whereas viral RNA and DNA should be of uniform length and composition; (3) the lethargy that characterizes what is considered ‘HIV replication’ excludes the possibility that replicative mutation can explain the wide HIV genetic variation; and (4) no one has produced a whole ‘HIV RNA’ molecule or a complete ‘HIV DNA’ strip, offering instead as the ‘HIV genome’ cobbled together bits of genetic material ... ‘HIV’ RNA and DNA haven’t been shown to code for what are claimed to be the HIV proteins, and all the ‘HIV’ genes are very similar to genetic sequences common to all humans. (Philpott, 1997)
When ‘HIV DNA’ shows up, it does so only in a tiny fraction of T-cells. For Duesberg, this means that HIV infects too few cells to cause any disease. But if HIV is so lethargic as to infect only a few cells, how can its amazing variability be explained? The Perth Group proposes that ‘HIV DNA’ originates from the rearrangement of normal cellular DNA sequences, and the fact that each one originates independently in each cell where it is found explains why ‘HIV’ DNA strips are always of varying length and composition. The chemical stimulants (often PHA) added to cell cultures to induce phenomena that are claimed to prove ‘HIV’ infection (retrovirus-looking objects plus certain proteins that may or may not be associated with them) are all oxidizing agents.
Duesberg and others argue that since the ‘HIV’ genome can be cloned, this proves that ‘HIV’ exists. But the simple fact that any DNA molecule can be cloned tells us nothing about the origin of that molecule (Perth Group, 1999). The only way to prove that a specific DNA sequence belongs to a specific virus is by isolating that virus and determining its genome. Molecular cloning is not a valid substitute for isolation, and cannot be considered proof for the discovery of a retrovirus.
According to microbiologist Phyllis E. Pease (2005), electron microscope work shows that particles previously assumed to be ‘HIV’ closely resemble cell-wall-deficient bacteria (such as mycoplasmas), both in shape and in variation of size. Such bacteria can transfer DNA from an outside source into someone’s own cells, and the altered cells might then attack normal cells, giving rise to autoimmune conditions such as rheumatoid arthritis and AIDS. As Pease says, there is ‘a considerable amount of pressure on research workers to direct and interpret their findings in a way that encourages the renewal of their grants’, and the present generation ‘has been taught that the cause of AIDS has been settled as a self-evident truth ... and that anyone who dares not accept it is mad, bad or both’ (p. 112).
In 2014, the public health journal Frontiers in Public Health published an article setting out the case against the HIV=AIDS hypothesis (Patricia Goodson, 2014). After receiving complaints from gatekeepers of the AIDS cult, the journal reclassified the article as an ‘opinion’, rather than a ‘hypothesis and theory’ article. The article continued to be widely read, and after further pressure was applied, the journal retracted it in 2019, on the grounds that it presents ‘a potential public health risk’, though the article has not been removed from its website. Such antiscientific practices testify to the weakness of the HIV/AIDS belief system.
There are many risk factors that can impair the immune system. Recreational drug use is the common denominator for over 95% of all American and European AIDS patients, including male homosexuals (Bialy, 2004, p. 186). Although two-thirds of all AIDS cases in the developed world involve gay men, only a small percentage of them have fallen victim to AIDS, namely those leading the fast-track lifestyle (which emerged in the 1970s), characterized by widespread use of recreational drugs, high levels of promiscuity and venereal disease, and overuse of antibiotics. Surveys have found that 93% to 100% of the gay men in question used drugs such as cocaine, heroin, poppers, amphetamines (‘speed’), barbiturates, marijuana, ethyl chloride, LSD, phencyclidine (PCP), and quaaludes.
At one time, 95% of gay men in major urban areas like Los Angeles, New York and San Francisco used poppers – volatile nitrite inhalants that dilate blood vessels and relax muscles, facilitating anal sex and heightening orgasm. Nitrite inhalants are potent oxidizing, immune-suppressive agents; they cause genetic mutations, cancer, lung damage and anaemia. Yet in the early 1980s US health authorities claimed they were harmless. They were often sold as ‘room odorizers’ or ‘incense’, and not subjected to any testing or regulation. Some gay publications received advertizing revenue from popper manufacturers, and refused to warn their readers of the dangers (Lauritsen & Wilson, 1986).
Nitrite use correlates strongly with Kaposi’s sarcoma (KS) and non-Hodgkin’s lymphoma, two AIDS-defining cancers found almost exclusively in this risk group. KS is also documented in HIV-negative gay men who used poppers (Maggiore, 2000, pp. 54-5). By 1991 only a quarter of gays used poppers, and the proportion of AIDS cases with KS fell from 50% in 1981 to 10% in 1991. KS remains an AIDS-defining disease, even though HIV researchers now accept that it is not caused by HIV, and has more to do with an overactive immune system than with immune deficiency.
Injection drug users account for 35% of all diagnosed AIDS cases. Only 10% of Americans diagnosed with AIDS cite heterosexual contact as their only risk; nearly half of them (4%) mention sexual relations with users of injection drugs, but most later admit taking drugs themselves. Over 80% of the mothers of babies diagnosed with AIDS acknowledge using injection drugs during pregnancy, which almost always results in intrauterine malnutrition (Maggiore, 2000, pp. 56-8). The remaining cases may be due to toxic medical treatments given in response to HIV-positive test results.
Only long-term drug consumption causes irreversible AIDS-defining diseases, whereas occasional or short-term drug use causes reversible diseases or no diseases at all. The long ‘latent period’ of HIV is a euphemism for the time needed to accumulate the drug dosage sufficient to severely damage the immune system. It takes 20 years of smoking to acquire irreversible lung cancer or emphysema, and 20 years of drinking to acquire irreversible liver cirrhosis. If it takes about 10 years of nitrites, heroin, amphetamines or cocaine to develop AIDS, then AIDS in the United States is a consequence of the drug epidemic that started in the late 1960s during the Vietnam War. The much more toxic ‘anti-HIV’ drug AZT can cause AIDS within a year. The virus hypothesis fails to explain why AIDS is linked to drugs or why the risk of AIDS depends on the lifetime dosage of drugs. The fact that 85% of AIDS-causing drugs are used by males, particularly sexually active homosexuals between 25 and 49 years of age, explains why about 80% of western AIDS patients are males (Duesberg, 1996).
Mainstream anti-AIDS campaigns focus on safe sex and clean needles while turning a blind eye to the well-documented health effects of long-term drug use. Duesberg (1996, p. 410) writes: ‘These strategies are based on the bias of the current medical establishment that recreational drugs are basically not toxic and that all diseases of drug addicts are caused by deadly viruses and microbes.’ There has never been any evidence that most intravenous drug users share needles. Clean, sterile needles may be better than dirty ones, but it is the contents of the syringe that are the main problem. Distributing sterile needles may even encourage further drug abuse, and surveys show that those who do not share needles can test HIV-positive more frequently than those who do.
A positive HIV test gives rise to psychological risk factors: belief in the inevitability of AIDS creates chronic anxiety, stress, panic and despair, which undermine health. ‘AIDS counsellors’ used to urge their clients to prepare for an early death as soon as they tested HIV-positive. Furthermore, almost everyone with an HIV-positive status consumes anti-HIV drugs that are highly toxic, ruin the immune and digestive systems, and cause several AIDS-defining illnesses. These drugs become harmful and even deadly when used on a daily basis. Duesberg argues that if toxic AIDS therapies were discontinued, thousands of lives could be saved virtually overnight.
As far as sexual practices are concerned, the Perth Group highlights evidence that semen is one of the most potent biological oxidants (a property essential for fertilization of the ovum), and is both carcinogenic and immunosuppressive (Papadopulos et al., 2010, 2017). Numerous studies have shown that homosexual men exposed to frequent, unprotected, receptive anal sex are at high risk of testing positive and subsequently developing AIDS, whereas no such risk is associated with the active (semen-donating) male. The number of instances of passive anal sex shows a higher correlation with testing HIV-positive than does the number of sexual partners.
For heterosexuals, too, the only sexual risk factor for a positive antibody test is passive anal intercourse. In contrast to vaginal intercourse, anally deposited semen is retained and absorbed into the bloodstream, because the rectum is lined by a single layer of absorptive cells, whereas the vagina has a multilayered, skin-like protective lining. Absorption of semen is also facilitated by rectal and colonic damage during anal intercourse. Condoms can eliminate this risk, but the condom breakage rate during anal sex is 0.5% to 8%.
The introduction of foreign protein into a person’s body triggers an immune response. That is why blood donors are matched as closely as possible to recipients, and recipients of organ transplants have to be given immune-suppressive drugs. Haemophiliacs and blood transfusion recipients make up 2% of adult AIDS cases in the United States. Factor VIII (a blood-clotting agent) and blood transfusions are immune-suppressive. Due to the serious conditions for which transfusions are necessary and their harmful effects on the body, half of all HIV-negative transfusion recipients die within a year of receiving a transfusion. So it is blood itself, not the ‘HIV’ it may contain, that causes harm. Those who test HIV-positive are additionally subjected to toxic drug treatments.
In stark contrast to the United States and Europe, AIDS cases in the developing world are found almost exclusively among non-drug-using heterosexuals. Mainstream AIDS experts can offer no plausible reason why AIDS would spread primarily through drug-free heterosexual contact only outside the US and Europe. Christine Maggiore writes:
A coherent explanation for AIDS cases in developing areas of the world is the well-known health risks in these countries – widespread poverty and malnutrition; lack of clean water, a regular food supply, and sanitary living conditions; limited access to medical care; endemic diseases such as tuberculosis, malaria, and parasitic infections that manifest in conditions identical to AIDS; and the practice of diagnosing AIDS based on a nonspecific set of clinical symptoms.
Although HIV tests are not required for AIDS diagnosis in many parts of world, widespread exposure to hepatitis, tuberculosis, leprosy, malaria and other conditions are more than sufficient to account for positive results on the nonspecific HIV antibody tests. (2000, pp. 58-9)
The money spent on antiretroviral drugs would be better spent on improving sanitation and access to safe drinking water, the absence of which kills about 1 million people a year.
Contrary to popular mythology, it is not necessary to consume antiretroviral drugs to avoid dying of AIDS. Even mainstream researchers admit that ‘some people with HIV who for years and even decades show extremely low levels of the virus in their blood never progress to full-blown AIDS and remain symptom free even without treatment’ (sciencedaily). In addition, thousands of HIV-positive men, women and children throughout the world have remained free of AIDS for decades by quitting toxic AIDS medications, stopping or significantly reducing their use of recreational drugs, and pursuing health-enhancing practices such as proper nutrition, adequate rest and regular exercise. Because these people are defying the HIV=AIDS=Death paradigm, they are rarely mentioned in mainstream literature.
Christine Maggiore was diagnosed HIV-positive in 1992 and was given five to seven years to live, even though she had no symptoms of illness. At first she became an AIDS activist, but a series of conflicting HIV test results in 1993 inspired her to question official HIV/AIDS dogma and led her to become an AIDS dissident. She avoided antiretroviral therapy and remained healthy long after she was supposed to have died. In 1995 she founded Alive & Well AIDS Alternatives to support others like her.
First-hand accounts by many long-term survivors or ‘nonprogressors’ can be found in her book What If Everything You Thought You Knew About AIDS Was Wrong? This is what some of them have to say:
The decision to stop taking the drugs is a difficult one in the face of pressure from doctors, the propaganda from the pharmaceutical companies and the organizations funded by them, and all the media hype. You really have to believe in yourself and take responsibility for your own life out of their hands and into your own, and just let go. ... Once you take that leap of faith you realize there is life without the drugs. (p. 123)
I have taken responsibility for my own life and have not allowed someone in a white lab coat to do it for me. Had I chosen that path they offered me, I know I would be dead. I’m a survivor because someone had the guts to tell me the truth about the HIV=AIDS=Death lie. It’s bad science in the hands of bad government. (p. 111)
In 1996 I got married – five years after I was supposed to be dead! I’m very alive and healthy ... Fear and isolation is what really kills people who test HIV positive. I fully believe that the HIV=AIDS hypothesis is a violation of our rights to life and liberty, and that ignorance is the real epidemic. (p. 95)
Henry H. Bauer, ‘Demographic characteristics of HIV: I. How did HIV spread?’,
Journal of Scientific Exploration, 19:4, 2005, pp. 567-603
--------------------- ‘Demographic characteristics of HIV: II. What determines the frequency of
positive HIV tests?’, Journal of Scientific Exploration, 20:1, 2006a, pp. 69-94
--------------------- ‘Demographic characteristics of HIV: III. Why does HIV discriminate by
race?’, Journal of Scientific Exploration, 20:2, 2006b, pp. 255-288
Henry H. Bauer, The Origin, Persistence and Failings of HIV/AIDS Theory, Jefferson, McFarland & Company, 2007
Henry H. Bauer, The case against HIV, December 2017
Henry H. Bauer, ‘Racial disparities in HIV tests: better explanation needed’, Journal of the American Physicians and Surgeons, v. 29, 2024, pp. 55-7
J.W. Bess et al., ‘Microvesicles are a source of contaminating cellular proteins found in purified HIV-1 preparations’, Virology, v. 230, no. 1, 1997, pp. 134-44
Harvey Bialy, Oncogenes, Aneuploidy and AIDS: A scientific life and times of Peter H. Duesberg, Cuernavaca, Mexico, Institute of Biotechnology, Autonomous National University of Mexico, 2004
Rebecca Culshaw, Science Sold Out: Does HIV really cause AIDS?, Berkeley, CA, North Atlantic Books, 2007
Etienne de Harven, Problems with isolating HIV, address to the European Parliament, 2003
Etienne de Harven, ‘Human endogenous retroviruses and AIDS research: confusion, consensus, or science?’, Journal of American Physicians and Surgeons, v. 15, 2010, pp. 69-74
Peter H. Duesberg, Inventing the AIDS Virus, Washington, DC, Regnery, 1996
Peter Duesberg, Claus Koehnlein and David Rasnick, ‘The chemical bases of the various AIDS epidemics: recreational drugs, anti-viral chemotherapy and malnutrition’, Journal of Bioscience, v. 28, 2003, pp. 383-412
Peter Duesberg et al., ‘HIV-AIDS hypothesis out of touch with S. African AIDS – a new perspective’, Medical Hypotheses, 2009 (withdrawn)
Peter Duesberg et al., ‘AIDS since 1984: no evidence for a new, viral epidemic – not even in Africa’, Italian Journal of Anatomy and Embryology, v. 116, 2011, pp. 73-92
Celia Farber, ‘Out of control: AIDS and the corruption of medical science’, Harper’s Magazine, March 2006
A.S. Fauci and J. Whitescarver, ‘The 30th anniversary of the first reported cases of AIDS’, NIH Medline Plus, v. 6, 2011, pp. 10-12
P. Gluschankof et al., ‘Cell membrane vesicles are a major contaminant of gradient-enriched human immunodeficiency virus type-1 preparations’, Virology, v. 230, 1997, pp. 125-33
Patricia Goodson, ‘Questioning the HIV/AIDS hypothesis: 30 years of dissent’, Frontiers in Public Health, v. 2, 2014, article 154 (retracted 2019)
D.J. Griffiths, ‘Endogenous retroviruses in the human genome sequence’, Genome Biology, v. 2, no. 6, 2001, 1017.1-1017.5
Neville Hodgkinson, ‘AIDS: scientific or viral catastrophe?’, Journal of Scientific Exploration, 17:1, 2003, pp. 87-120
Neville Hodgkinson, ‘Review essay on AIDS, Cancer and Arthritis: A new perspective by Phyllis Evelyn Pease’, Journal of Scientific Exploration, 23:3, 2007, pp. 595-605.
Neville Hodgkinson, The six mistakes that created and sustained ‘HIV’, 2017, theperthgroup.com
James P. Hogan, Kicking the Sacred Cow: Questioning the unquestionable and thinking the impermissible, Riverdale, NY, Baen, 2004
C. Johnson, ‘Whose antibodies are they anyway?’, Continuum, v. 4, no. 3, 1996, pp. 4-5
Robert F. Kennedy, The Real Anthony Fauci: Bill Gates, Big Pharma, and the global war on democracy and public health, Skyhorse, 2021
Stefan Lanka, ‘HIV: reality or artefact?’, Continuum, v. 3, no. 1, April/May 1995, pp. 4-9
Stefan Lanka, Interview: Challenging both mainstream and alternative AIDS views, December 1998, virusmyth.com
John Lauritsen, ‘AIDS: a death cult’, Gay and Lesbian Humanist, winter 2003-2004 (2007 version)
John Lauritsen, History of the controversy, Rethinking AIDS Conference, Oakland, California, 7 November 2009
John Lauritsen, The ‘AIDS’ hoax and gay men, International Conference, AIDS: Knowledge and Dogma, Vienna, Austria, 17 July 2010
John Lauritsen and Hank Wilson, Death Rush: Poppers & AIDS, New York, Pagan Press, 1986
Christine Maggiore, What If Everything You Thought You Knew About AIDS Was Wrong?, Studio City, CA, American Foundation for AIDS Alternatives, 4th ed., 2000
Donald W. Miller, HIV/AIDS: Unmasking falsehood, bringing truth to light, August 2015
Kary Mullis, Dancing Naked in the Mind Field, New York, Vintage, 1998
N.S. Padian et al., ‘Heterosexual transmission of human immunodeficiency virus (HIV) in Northern California: results from a ten-year study’, American Journal of Epidemiology, v. 146, no. 4, 1997, pp. 350-7
Eleni Papadopulos-Eleopulos, An analysis of evidence for the existence of HIV, evidence to the Supreme Court, Adelaide, 2006, theperthgroup.com
Eleni Papadopulos-Eleopulos et al., The Perth Group revisits the existence of HIV, International Conference on HIV/AIDS, Ekaterinburg, Russia, 2008, theperthgroup.com
Eleni Papadopulos-Eleopulos et al., AIDS – Sexually transmitted or sexually acquired?, 2010, theperthgroup.com
Eleni Papadopulos-Eleopulos et al., A commentary on immune deficiency and AIDS, November 2016, theperthgroup.com
Eleni Papadopulos-Eleopulos et al., HIV – A virus like no other, July 2017, theperthgroup.com
B.A.I. Payne et al., ‘Mitochondrial aging is accelerated by anti-retroviral therapy through the clonal expansion of mtDNA mutations’, Nature Genetics, v. 43, no. 8, 2011, pp. 806-10
Phyllis Evelyn Pease, AIDS, Cancer and Arthritis: A new perspective, Birmingham, Phyllis Evelyn Pease, 2005
Perth Group, Email correspondence with Robin Weiss, 1999
Perth Group, The emperor’s new virus?, September 2011
Perth Group (2016a), Cellular oxidation and AIDS, November 2016
Perth Group (2016b), Some comments on the use of animal models to prove the HIV theory of AIDS, November 2016
Paul Philpott, ‘The isolation question’, Reappraising AIDS, June, July, August 1997
Janine Roberts, Fear of the Invisible: An investigation of viruses and vaccines, HIV and AIDS, Bristol, Impact Investigative Media Productions, 2nd ed., 2009
B. Rodríguez et al., ‘Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection’, Journal of the American Medical Association, v. 296, no. 12, 2006, pp. 1498-1506
Joan Shenton, Positively False: Exposing the myths around HIV and AIDS, London, Immunity Resource Foundation, 2nd ed., 2015
Mike Stone, HIV transmission rare or non-existent?, 2021, viroliegy.com
Craig Timberg, ‘U.N. to cut estimate of AIDS epidemic – population with virus overstated by millions’, Washington Post Foreign Service, 20 November 2007
Websites:
theperthgroup.com
hivskeptic.wordpress.com (Henry Bauer)
rethinkingaids.com
Treatment Information Group
aliveandwell.org
davidrasnick.com
paganpressbooks.com (John Lauritsen)
duesberg.com
virusmyth.com
tig.org.za/Brink_bio.htm (Anthony Brink)
Reclaiming our health: germ theory exposed
Mass psychosis and the power of thought
Ozone, influenza and the causes of disease
Health and disease: theosophical quotations